Iron
Iron
Iron is a fundamental mineral involved in energy metabolism, oxygen transport, cognitive function and immunity.
Athlete infographics have been developed for the information of athletes under the direct guidance of a sports dietitian. Sports dietitians have expert knowledge of sports supplements and their potential application in an athletes broader health and performance nutrition strategies. Always engage with a sports dietitian when considering the use of any supplement. https://www.sportsdietitians.com.au/#find-sports-dietitian, opens in a new tab
- Iron is a fundamental mineral involved in energy metabolism, oxygen transport, cognitive function and immunity.
- Almost two-thirds of the body’s iron is found in haemoglobin in circulating erythrocytes, with smaller amounts in ferritin and myoglobin.
- The body cannot produce its own source of iron and therefore it relies on absorbing the iron we consume as part of our diet or supplements. The recommended daily intakes of iron for adults are:
- ♂ - 8 mg per day
- ♀ - 18 mg per day (pre-menopause)
- Athletes are more susceptible to iron deficiency due to the greater iron demand associated with exercise, and the finite opportunity they have to replenish stores from food sources. Some high-risk athlete populations include:
- Female athletes (due to additional iron lost during menses).
- Endurance athletes, including those training at altitude (perhaps due to the greater demand on oxygen transport mechanisms).
- Vegetarian and Vegan athletes (since less iron is absorbed from plant sources).
- Athletes in Low Energy Availability.
- Compromised iron levels are typically associated with symptoms of lethargy and fatigue. In athletes, it may also manifest in reduced training and performance outcomes or a suppressed ability to respond/adapt to training stimuli.
- Iron deficiency is an issue that progresses in severity because of a negative iron balance. Early stages, known as iron deficiency non-anaemia (IDNA), occur when ferritin stores are depleted without significant impact on haemoglobin concentrations. The most severe stage, iron deficiency anaemia (IDA), presents when both iron stores and haemoglobin are depleted.
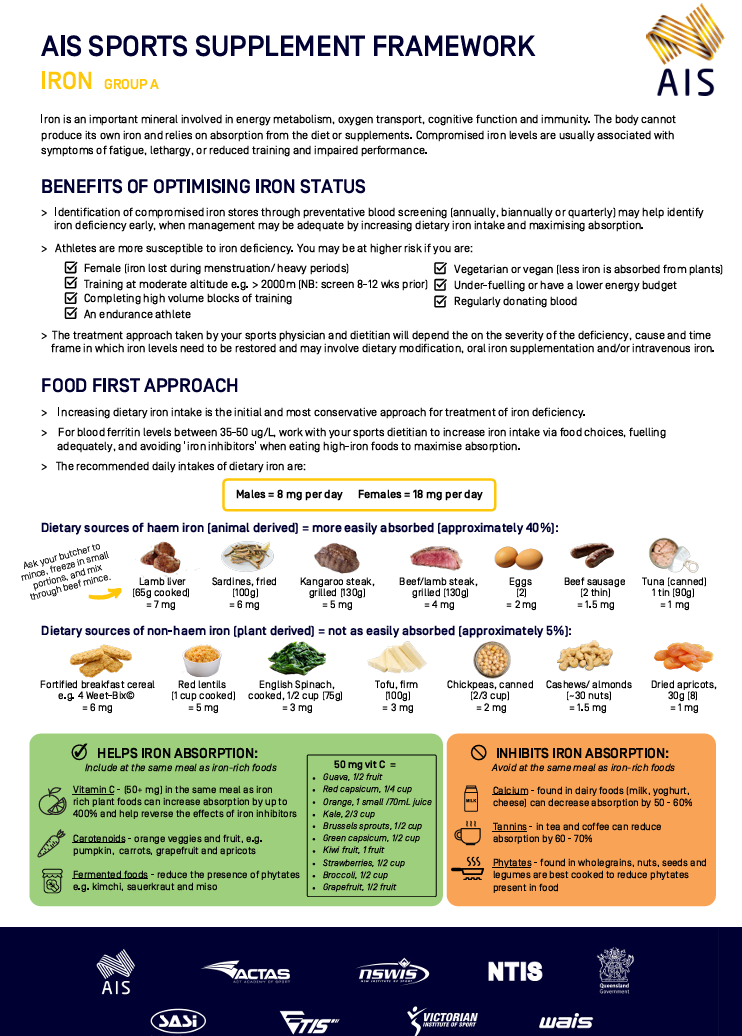
- Treatments for an iron deficiency range from nutritional support, oral iron supplementation, and intravenous iron approaches, depending on the severity of the issue and the athlete patient history. Increasing dietary iron intake is the initial and most conservative treatment for iron deficiency. Some examples of haem (animal derived) and non-haem (plant derived) sources of dietary iron.1
- Oral iron supplements are the following avenue of treatment and are typically provided as ferrous salts: ferrous fumarate, ferrous sulphate or ferrous gluconate.
- Ferrous sulphate preparations (e.g. FerroGrad®) containing ~100 mg elemental iron are the established and standard treatment for depleted iron stores. The total amount of elemental iron contained in the supplement should be checked to ensure that the specific target dose is achieved.
- Controlled-release iron formulations (e.g. Maltofer®) may be used if ferrous salts are not well tolerated by the athlete.
- Intravenous iron should only be considered in consultation with a sports physician. The efficacy of this approach appears best when IDA is present – i.e. when both ferritin stores and haemoglobin are compromised.
- Physicians are guided by the following outline when considering the frequency of iron blood screening for athletes.2
- Early identification of compromised iron stores (in the IDNA phase) is important since it allows athletes to consider nutritional and supplementation options with their physician and/ or accredited sports dietitian to prevent progression to IDA.
Figure 1. Framework of considerations for the frequency of iron blood screening in athlete populations.
Image text
Considerations and frequency of iron blood screening for athletes
Variables to be considered.
- Minimum: serum ferritin, hemoglobin concentration, transferrin saturation.
- Desirable: Serum soluble transferrin receptor, hemoglobin mass, C-reactive protein.
Standardisation of blood collection.
- Time of day: Preferably in the morning.
- Hydration state: Hydrated preferably assessed by waking urinary specific gravity (<1.025).
- Low to moderate activity in the proceeding 24 hours, including no muscle-damaging exercise (e.g. eccentric) in 2-3 days prior.
- No signs of sickness or infection.
Annually
- No history of iron deficiency.
- No history of irregular/excessive menses or amenorrhea.
- No reports of fatigue after extended rest.
- Strength/power-based sports with minimal endurance component.
- No iron-related dietary restrictions.
- No evidence of low energy availability.
- No intention to undertake hypoxic training in the next 12 months.
- No underlying pathology (e.g. coeliac or Crohn’s disease).
Biannually
- Female.
- Previous history (≥24 months) of iron depletion (e.g. Stage 1).
- Previous history (≥24 months) of irregular/excessive menses.
- Intention to undertake high training loads especially in endurance and team-based sports.
- Minimal (or zero) reports of prolonged fatigue after extended rest.
- No iron-related dietary restrictions (e.g. non-vegetarian, non-vegan).
- No evidence of low energy availability.
- Intention to undertake hypoxic training in the next 12 months.
Quarterly
- Any recent history (<24 months) of iron depletion/deficiency (Stage 1, 2, or 3) irrespective of sex.
- Any evidence of irregular/excessive menses or amenorrhea.
- High training loads in endurance and team-based sports.
- Reporting prolonged fatigue/lethargy even after extended rest.
- Reduced work capacity during training.
- Unexplained poor athletic performance.
- Individuals restricting sources of dietary iron (e.g. vegetarian and vegan) or overall caloric intake.
- Any evidence of low energy availability.
- Intention to undertake hypoxic training in the next 6 months.
This figure has been adapted from Sim et. al.2
- Below is a framework to guide practitioners towards optimal treatment protocols for iron deficient athletes, diagnosed via haematological indices.1
- Iron supplements should only be taken under medical supervision as part of an integrated iron management program, which includes dietary assessment and enhancement of dietary iron intake.
- Current research suggests that a daily dose of 100 mg of elemental iron (or every second day if GI upset is present) for 8-12 weeks can significantly improve ferritin stores.3,4,5 This should be confirmed via a subsequent blood test.
- Consuming the oral iron supplement in the morning, as close to exercise as possible, may result in a greater level of iron absorption.6
Figure 2. Framework to guide practitioners towards optimal treatment protocols for iron deficient athletes, diagnosed via haematological indice
Image text
Athlete blood screening
[left hand side]
IDNA
- sFer <35 µg·L-1·
- [female symbol] [Hb] 120 – 155 g·L-1·
- [male symbol] [Hb] 135 – 175 g·L-1·
Oral iron supplementation (4-12 weeks)
- 100 mg oral iron (ferrous salt) daily in the morning If negative GI side-effects experienced
- 100 mg oral iron (ferrous salt) on alternate mornings If negative GI side-effects persist
- 60 mg (or tolerable dose) oral iron on alternate mornings
OR
- mg controlled release oral iron on alternate mornings
Athlete intolerant or not responding to oral iron treatment
[middle]
Dietary assessment/intervention with an accredited sports dietitian
[right]
IDA
- sFer <12 µg·L-1·
- [female symbol] [Hb] <120 g·L-1·
- [male symbol] [Hb] <135 g·L-1·
IV treatment
Note: Individual responses to IV treatment vary. Follow up blood screen at 1 & 6-months post-treatment recommended.
[key]
Key
- - - Medical professional’s discretion
This figure has been adapted from McCormick et. al.1
- The absorption of oral iron supplements is enhanced by consuming it with a source of vitamin C (~50-100 mg). This can be achieved by choosing a supplement in which Vitamin C is also provided, or by consuming it with an appropriate (e.g. citrus) fruit or juice. Factors that interfere with iron absorption such as calcium (dairy) and tannins (tea and coffee) should be avoided for an hour each side of the time of consumption of the supplement.
- Examples of both inhibitors and promoters of non-haem iron absorption1 are presented in Table 1
Table 1. Dietary factors that either enhance or inhibit iron absorption.
Inhibitors of non-haem iron absorption | Promotors of non-haem iron absorption | |||
|---|---|---|---|---|
Phytates | Found in whole-grain cereals, legumes, nuts and seeds | Vitamin C (ascorbic acid) | Aim 50+ mg. Found in citrus fruit (e.g. oranges, kiwifruit), broccoli, tomato, capsicum | |
Polyphenols/ phenolic compounds | Found in tea (herbal and non-herbal), coffee, red wine and chocolate (cocoa) | Carotenoids | Found in pumpkin, carrots, grapefruit and apricots | |
Calcium | Found in dairy products (e.g. yoghurt, milk, cheese) and multivitamin supplements | Fermented foods | Fermentation reduces the presence of phytates; e.g. sauerkraut, kimchi and miso | |
Other minerals | Zinc and manganese (compete for intestinal absorption) | Cooking your food | Reduces the phytates present in food |
- If an athlete is undertaking specific altitude training, a pre-training screen of iron status is advised. This should be done with enough time (i.e. 8-12 weeks prior) to allow correction of iron depletion (IDNA or IDA) to be achieved prior to the start of the altitude training program.
- Athletes who have ferritin levels of 50-100 μg·L-1 (i.e. just above the levels traditionally considered to represent iron depletion) might consider taking an oral iron supplement (~100 mg daily or alternate day, as above) for two weeks prior to the start of altitude training and throughout the training program, since there is evidence that this supports greater adaptation to the altitude stimulus. Note: IV iron supplementation does not appear to improve the benefits of altitude adaptation more than oral supplementation.4,7,8
Failure to address dietary issues or other underlying causes of the iron deficiency
- Iron supplementation does not address dietary issues. Dietary counselling in the early investigation phase of treatment should be provided via a referral to an accredited sports dietitian.
- Where possible, the underlying cause for iron deficiency should be established so that it can be addressed. In some circumstances, a medical issue may need to be corrected.
Risk of iron overload or other medical issues
- Excessive iron intake in some athletes may lead to iron overload. People with haemochromatosis should avoid iron supplementation, since extremely high iron levels can be toxic to the body’s organs. Further information can be obtained from a sports doctor.
- Intravenous and intramuscular iron supplementation carries a risk of anaphylactic shock, and problems due to the use of needles.
Risk of gastrointestinal upset
- Some oral iron preparations cause gastrointestinal upset including constipation. Supplementation strategies such as ‘every second day’ approaches have been shown to reduce this gastrointestinal response, without compromising the supplements efficacy5 over time (8-12 weeks).
Sports Dietitians Australia www.sportsdietitians.com.au/iron, opens in a new tab
Supplement safety information www.sportintegrity.gov.au/what-we-do/anti-doping/supplements-sport, opens in a new tab
- McCormick R, Sim M, Dawson B, Peeling P. (2020). Refining treatment strategies for iron deficient athletes. Sports Med, 50(12), 2111-2123.
- Sim M, Garvican-Lewis LA, Cox GR, Govus A, McKay AKA, Stellingwerff T, Peeling P. (2019). Iron considerations for the athlete: a narrative review. Eur J Appl Physiol, 119(7), 1463-1478.
- Dawson B, Goodman C, Blee T, Claydon G, Peeling P, Beilby J, Prins A. (2006). Iron supplementation: oral tablets versus intramuscular injection. Int J Sport Nutr Exerc Metab, 16(2), 180-6.
- Garvican LA, Saunders PU, Cardoso T, Macdougall IC, Lobigs LM, Fazakerley R, Fallon KE, Anderson B, Anson JM, Thompson KG, Gore CJ. (2014). Intravenous iron supplementation in distance runners with low or suboptimal ferritin. Med Sci Sports Exerc, 46(2), 376-85.
- McCormick R, Dreyer A, Lester L, Sim M, Goodman C, Dawson B, Peeling P. (2019a). The efficacy of daily and alternate day oral iron supplementation in iron depleted athletes. Unpublished data.
- McCormick R, Moretti D, McKay AKA, Laarakkers CM, Vanswelm R, Trinder D, Cox GR, Zimmerman MB, Sim M, Goodman C, Dawson B, Peeling P. (2019b). The Impact of Morning versus Afternoon Exercise on Iron Absorption in Athletes. Med Sci Sports Exerc, 51(10), 2147-2155.
- Garvican-Lewis LA, Govus AD, Peeling P, Abbiss CR, Gore CJ. (2016). Iron Supplementation and Altitude: Decision Making Using a Regression Tree. J Sports Sci Med, 15(1), 204–205.
- Govus AD, Garvican-Lewis LA, Abbiss CR, Peeling P, Gore CJ. (2015). Pre-Altitude Serum Ferritin Levels and Daily Oral Iron Supplement Dose Mediate Iron Parameter and Hemoglobin Mass Responses to Altitude Exposure. PLoS One, 10(8).