Fish oils
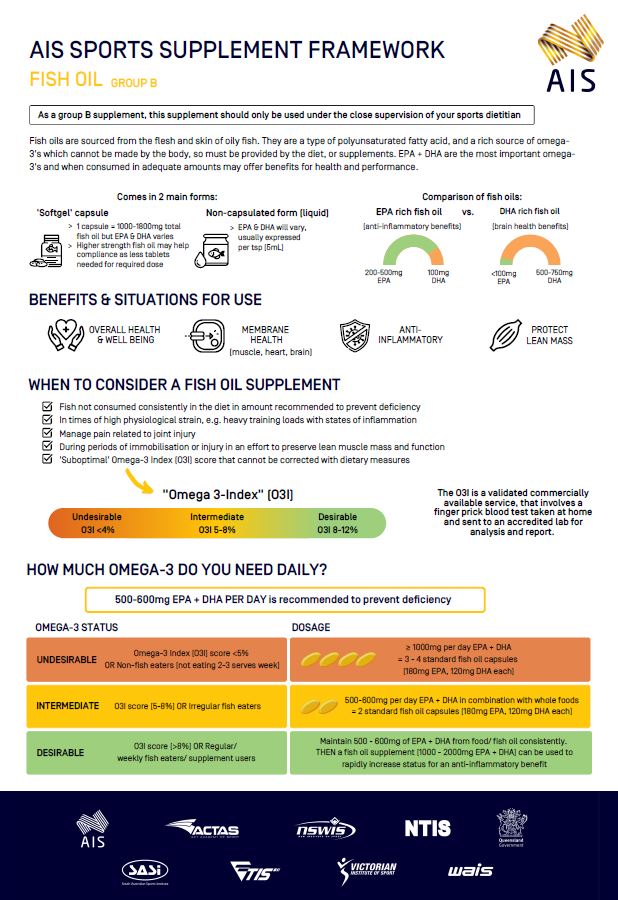
Fish Oil
(Omega-3 Fatty Acids - EPA and DHA)
Fish (or marine) oil comprises of >50 fatty acid isomers. These include the major groupings of saturated, monounsaturated and polyunsaturated fatty acids (divided into omega-6 and omega-3).

36194_Sport-supplement-fact-sheets-Fish-oil-v3.pdf
Athlete infographics have been developed for the information of athletes under the direct guidance of a sports dietitian. Sports dietitians have expert knowledge of sports supplements and their potential application in an athletes broader health and performance nutrition strategies. Always engage with a sports dietitian when considering the use of any supplement. https://www.sportsdietitians.com.au/#find-sports-dietitian, opens in a new tab
- Fish (or marine) oil comprises of >50 fatty acid isomers. These include the major groupings of saturated, monounsaturated and polyunsaturated fatty acids (divided into omega-6 and omega-3). The relative composition varies according the type of fish from which the oil is derived.
- By far the most abundant of the fatty acids in fish oil, and the basis for its consumption, are the omega-3 polyunsaturated fatty acids; Eicosapentaenoic Acid [EPA; 20:5n-3] and Docosahexaenoic Acid [DHA; 22:6n-3].
- When EPA and DHA are provided in the diet, through either food such as fish or as a supplemental fish oil, the fatty acid profiles of the plasma, whole blood and red blood cells membranes are modified. These increased concentrations of EPA and DHA reduce the overall omega-6 / omega-3 ratio and specially the arachidonic acid (AA) / eicosapentaenoic acid (EPA) ratio in favour of anti-inflammation.
- Most notably, these changes in the proportion of EPA and DHA of the red blood cell membrane, represent the long-term dietary intake of these polyunsaturated fatty acids and act as a biomarker for other tissues. For example, skeletal muscle, heart and brain avidly incorporate membrane DHA. Remodelling of these membranes has been shown to…
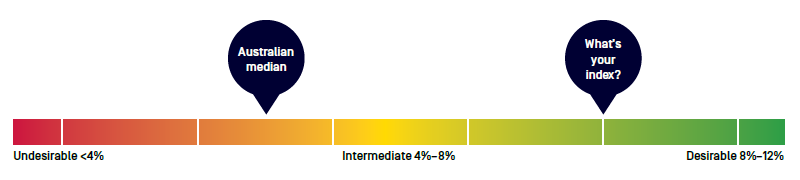
- Improve the omega-3 status: The Omega-3 Index (O3I) is the relative sum of EPA% + DHA% in the red blood cell membrane. It is desirable for the O3I to be >8%. As a consequence of increasing the O3I, the omega-6/omega-3 ratio will be reduced <5 and the AA / EPA <11, which are promoted ratios for cardio-protection (O3I) and anti-inflammation (omega-6 / omega-3 and AA/EPA).1,2
- Modify physiological function: Preliminary evidence supports that an improved omega-3 status i). May reduce physiological strain, through for example, a reduction in heart rate1,3 ii). Aid in the recovery process via an anti-inflammatory (EPA) and pro-resolvin effects (DHA) (which turn off the inflammation process)4 and iii). Potentially protect against a reduction in muscle protein synthesis during periods of immobilisation, such as injury.5
- The most common form of fish oil is the capsule (or ‘softgel’) with a composition of gelatin, glycerine and purified water. In general, the standard total mass range for each capsule is 1000 – 1500 mg At this total mass, each capsule provides a varied dose of the two key long chain omega-3 polyunsaturated fatty acids; EPA and/ or DHA.
- Fish oil can also be purchased in a non-capsulated form or bottled. The dose of EPA and DHA will also vary between brands, according to the fish stock. The quantity of long chain omega-3 fatty acids is usually described according to the volume of a teaspoon (5 mL). Table 1: Comparison of fish oils providing EPA and DHA
- The following table provides a comparison of the predominant types of commercially available fish oils. It is essential to check the content of the fish oil for the concentrations of the active components, EPA and DHA. In addition, the EPA and DHA are supplied in a variety of usual forms. Free fatty acids, natural triglycerides and re-esterified triglycerides tend to have the highest bioavailability.
- The standard western diet, largely devoid of consistent seafood consumption, means that the average intake of EPA and DHA, for an individual, is likely below the recommendations for avoiding a deficiency in omega-3 fatty acids. It is recommended that at least two servings per week of fatty fish are included in the diet, in addition to food sources that provide alpha-linolenic acid (ALA; 18:3n-3).
- The food first approach, as part of the overall diet, should always be considered. The following example servings of fish, provide varied amounts of the long chain fatty acids, EPA and DHA. For canned fish, always check the product description, as fish sources can vary in their content of EPA and DHA.
- Services are available commercially to determine the O3I. Athletes with a low dietary intake of EPA + DHA may benefit from tracking their improvements associated with the commencement of a supplement. A dry blood spot is collected (fasting state), from a self-conducted finger prick (in the home). The sample is sent via the mail to an internationally accredited pathology centre or university laboratory for analysis. A report is produced that includes a whole blood fatty acid profile, the O3I and the inflammatory ratios omega-6/omega-3 (target <5) and AA/EPA (target <11).
Figure 1: Omega-3 Index (red blood cell EPA + DHA%) with Australian median (estimated) value. The target is to elevate and thenmaintain an O3I >8% (green zone).
- The first objective, and overriding principle for correcting an omega-3 intake deficiency, is a consistent and long term provision of EPA and DHA in the diet. It is possible to achieve an optimal concentration of EPA and DHA in the circulation and the tissues using whole foods (as listed above). A combined EPA + DHA intake of 500-600 mg per day is the minimum target and careful planning of the diet is necessary to achieve this consistency. Alternately, for those with no intake or inconsistent dietary sources of omega-3, a daily supplement of 1-2 capsules per day (depending on the oil and brand) will achieve equivalent outcomes for modifying membranes.
- The second objective is to maximise the omega-3 status to aid physiological function of heart and muscle, particularly in times of high physiological strain and need for recovery. The preliminary, aggregated evidence, suggests that a combined EPA + DHA dose of ≥1000 mg per day is linked to reduced physiological strain (such as a reduction in heart rate), improvement of exercise induced inflammation response and possible preservation of muscle structure and function during specific conditions such as immobilisation.
- The following table summarises the key points to optimising, maximising and maintaining circulating and tissue concentrations of EPA and DHA.
Table 1: Summary of current evidence for fish oil consumption >
Timing | Consume with a mealConsuming the fish oil capsules in conjunction with a normal meal, maximises the EPA and DHA digestion and absorption.Once the omega-3 status is optimised (O3I >8%), missing or skipping several days of intake will have minimal impact. The EPA and DHA, which are taken up into the cells’ membranes, are maintained as incorporated fatty acids, on average for 2 weeks, even when omega-3 supplemental intake is withdrawn. |
|---|---|
A low omega-3 status (O3I <5%): non-fish eaters
An intermediate omega-3 status (O3I 5-8%): irregular fish eaters
An optimal omega-3 status (O3I >8%): regular / weekly fish eaters and long term fish oil supplement consumers
| |
Overall wellbeing / health: 500-600 mg per day of EPA + DHA Optimising muscle, heart and brain tissue membranes: 500-600 mg per day of DHA Anti-inflammation (EPA)/pro-resolving (DHA): 1000-2000 mg per day of EPA + DHA During periods of injury: consider increasing to >1000 mg per day of EPA +DHA |
Storage
- The long chain omega-3 fatty acids contained in fish oil are oxidisable. Most oils will contain the antioxidant, alpha tocopherol, to protect the EPA and DHA from degrading. It is best practice to make sure that capsules are in date, stored in the purchased container and kept in a consistently cool environment (a fridge is also fine) away from direct light.
Bleeding
- The European Food Safety Authority considers intakes up to 5 grams of fish oil per day safe.6 The EPA active component of fish oil can modify the coagulation properties of the blood involved bleeding. However, a recent randomised placebo-control trial reported no increased risk of peri-operative bleeding7 and a systematic literature review (of 52 studies) concluded that fish oil supplementation did not increase the risk of bleeding during or after surgery.8 In the advent that surgery is required, some pre-operative assessments will request information about current fish oil consumption.
Gastrointestinal discomfort, allergies and the vegan diet
- Research involving therapeutic doses (>5 g of total oil) have sometimes reported gastrointestinal discomfort, in a minority of participants. Consuming the fish oil (capsule) with other foods results in the digestion and absorption occurring alongside other macro and micronutrients. The capsules are also designed to dissolve slowly and in time for movement of the oil into the duodenum (small intestine). Consuming a non-capsulated fish oil product (usually a teaspoon of oil) without other foods, is more likely to result in reflux and after taste, although some of these non-capsulated oils are flavoured to improve palatability.
- A small proportion of the population are allergic to fish and seafood products. Before consuming, it is worth considering if this applies to each individual.
- Athletes consuming a plant based diet will most likely have a low omega-3 status (reflected by the O3I <4.5%). Although fish oil is avoided in the vegan diet, EPA and DHA can be sourced from algal oil and has been demonstrated to be effective in the wider population in raising the O3I.
Fish oil in combination capsules
- Several major brands combine fish oil with either anti-oxidants, such as curcumin, or vitamin D. To date, there are few studies published exploring the efficacy of combined capsules although some seem promising. For example, a combined fish oil and vitamin D supplement was reported to reduce the number of URTI symptom days in recreational athletes.9
- Krill oil also contains a good source of EPA and DHA. Krill oil differs from fish oil in that the major form of the long chain omega-3 fatty acids are phospholipids. This factor may improve membrane incorporation although studies in trained groups are limited.10 Krill oil also naturally contains the antioxidant astaxanthin which provides an opportunity combining their intake.
Global Organisation for EPA and DHA Omega-3 www.goedomega3.com, opens in a new tab
National Heart Foundation www.heartfoundation.org.au/getmedia/741b352b-1746-48f4-806a-30f55fddfad2/Health_Professional_QA_Fish_Omega3_Cardiovascular_Health.pdf, opens in a new tab
Supplement safety information www.sportintegrity.gov.au/what-we-do/anti-doping/supplements-sport, opens in a new tab
- Peoples, G. E., and McLennan, P. L. (2016) Chapter 10: Fish Oil for Physical Performance in Athletes in Fish and Fish Oils in Health and Disease. Editors Raatz S, Bibus D. USA, Elsevier Inc. ISBN 978-0-12-802844-5.
- Calder, P. (2013) Omega-3 polyunsaturated fatty acids and inflammatory processes: nutrition or pharmacology? Br J Clin Pharmacol. 75 (3); 645
- Macartney, M.J., et al. (2014) Intrinsic heart rate recovery after dynamic exercise is improved with increased omega-3 index in healthy males. BJN. 112, 1984–1992.
- Philpott, J. D. et al. (2018) Applications of omega-3 polyunsaturated fatty acid supplementation for sport performance. Res Sport Med, 27(2):219-237.
- McGlory, C., et al. (2019) The Influence of Omega-3 Fatty Acids on Skeletal Muscle Protein Turnover in Health, Disuse, and Disease. Frontiers in Nutr, 6; 144.
- European Food Safety Authority (2012) Scientific opinion on the tolerable upper intake level of eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA) and docosapentaenoic acid (DPA). EFSA J. 10:2815
- Akintoye, E, et al. (2018) Fish oil and perioperative bleeding. Circ Cardiovasc Qual Outcomes. 11:004584.
- Begtrup, KM, et al (2017). No impact of fish oil supplements on bleeding risk: a systematic review. Dan Med J. 64:1–11.
- Da Boit, M. et al. (2015) The effect of fish oil, vitamin D and protein on URTI incidence in young active people. Int J Sports Med. 36(5): 426-430.
- Daboit, M. et al (2015) The effect of krill oil supplementation on exercise performance and markers of immune function. Plos One. 1-14